

Why Now?
Hospice is an important and beneficial end-of-life service that provides care for the patient and family. But half of all patients who require hospice are on service for less than 21 days out of a six-month benefit. Learn more about how early intervention promotes better care and prevents crisis, and see what signs providers should look for.
4 Methodologies to Determine Hospice Eligibility
Patient meets Medicare administrative contractors disease-specific guidelines to help determine if a patient meets the clinical criteria for the Hospice Medicare benefit.
If a patient experiences acute symptoms that cannot be safely managed in the home or other residential setting, they may require a higher level of care called general inpatient (or GIP) care. GIP care may be provided in a contracted skilled nursing facility or a hospital. Once symptoms are under control, the patient may return to their home under the routine level of care.
- Deterioration in lab values
- Evidence of metastatic disease
- ER or hospital visits in last 6 months
- Unintentional weight loss
- Decline in functional status
Patients who meet most of the LCD guidelines may still be eligible for Hospice if they have a terminal illness with a prognosis of 6 months or less and have significant life limiting co-morbidities
- Dementia
- CRF
- COPD
- CHF
Patients who do not meet all the LCD guidelines but who still have a terminal illness with a prognosis of six months or less may still be eligible if their disease follows the normal course. An attending physician may consult with a Medical Director to review the patient’s status to determine eligibility.
Guidelines & Indicators
- Life limiting conditions with a prognosis of 6 months or less if the disease follows its normal course
- Patient elects the palliative measures over curative measures
- Physician in agreement with palliative measures over curative measures
- PPS score < 50%
- Increase in ER and hospital visits in last 6 months
- Falls or fractures in the last 6 months
Assisted Daily Living
Evidence by dependency in 3 of the 6 ADL’s
- Bathing
- Toileting
- Transfers
- Feeding
- Dressing
- Ambulation
Other Indicators of Decline
- Increased sleep or lethargy
- BMI of < 22
- Unintentional weight loss of 10%
- Decreasing serum albumin
- Cholesterol < 150
- Dysphasia or choking
- Impaired nutrition despite external use
A terminal illness condition not related to a single diagnosis is difficult to determine a primary reason for hospice eligibility. The following guidelines will assist you through determination:
- Rapid or observed decline in past three to six months
- Multiple emergency department visits with or without admission
- Recurrent urinary tract infections, pneumonia or other infections causing patient to decline
- Unwanted or non-reversible weight loss
Secondary Conditions
- Protein calorie malnutrition
- Mobility
- Cachexia
- Decubitus ulcers
- Muscle wasting
- Behavioral or cognitive decline over past six months
- Recurring infections
- Septicemia
- Other supporting documentation
- KPS < 40%
- BMI < 22% kg/m
This documentation of structural/functional impairments and activity limitations facilitate the selection or intervention strategies (palliative vs. curative) and provide objective criteria for determining the effects of such interventions. The documentation of these variables is thus essential in the determination of reasonable and necessary Medicare Hospice service.

The BMI is an attempt to quantify the amount of tissue mass (muscle, fat, and bone) in an individual, and then categorize that person as underweight, normal weight, overweight, or obese based on that value. Commonly accepted BMI ranges are underweight : under 18.5, normal weight: 18.5 to 25, over weight: 25 to 30, obese: over 30.

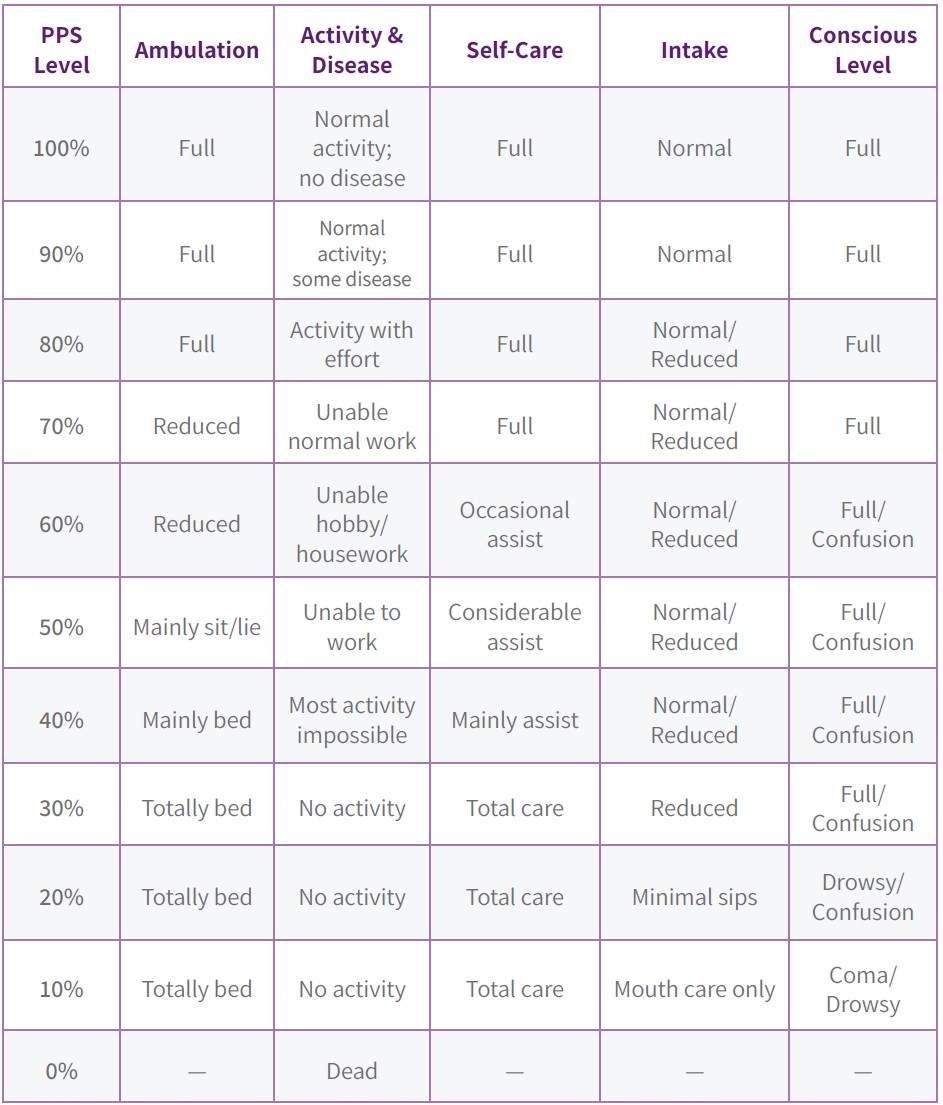
The Palliative Performance Scale Version Two (PPSV 2) is a tool for measurement of performance status in palliative care. The PPSV2 allows common language about performance status that is more relevant in palliative care than the Karnofsky Performance scale from which it is based.
A standard way of measuring the ability of patients to perform ordinary tasks. The Karnofsky Performance Scale scores range from 0 to 100. A higher score means the patient is better able to carry out daily activities. KPS may be used to determine a patient’s prognosis, to measure changes in ability to function or to decide if a patient could be included in a clinical trial.

- Symptoms of recurrent heart failure or angina at rest or discomfort with activity
- New York Heart Class IV-supporting clinical factors include discomfort/dyspnea at rest
- Ejection fraction of 20% or less with supportive data
- Multiple hospitalizations or emergency department visits within one year
- History of cardiac arrest or heart attack
- Frequent medication/dosage changes with patient already optimally treated with diuretics and vasodilators
Secondary Conditions
- Shortness of breath at rest
- Paroxysmal nocturnal dyspnea
- Awaiting heart transplant
- Lethargy
- Increased fatigue
- Liver enlargement
- Shortness of breath in a reclined position
- Dependent edema arrhythmias
- Cachexia diaphoresis
- Neck vein distension
Cardiac Agape Care
Registered nurse: will assess pain and other symptoms and implement ordered pain control measures
Social worker: will assess psychological, financial and emotional needs related to illness
Spiritual care counselor: will counsel, support and intervene related to spiritual care needs and wishes; will support with listening and presence
Home health aide: will support with activities of daily living and homemaker services
Volunteers: will support with companionship, errands and other activities
Functional Classification Scale in a Patient with Heart Disease
Doctors usually classify patients’ heart failure according to the severity of their symptoms. The table below describes the most commonly used classification system. It places patients in one of four categories based on how much they are limited during physical activity.
Class I
No limitation of physical activity. Ordinary physical activity does not cause undue breathlessness, fatigue or palpitations.
Class II
Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in undue breathlessness, fatigue or palpitations.
Class III
Marked limitation of physical activity. Comfortable at rest, but less than ordinary physical activity results in undue breathlessness, fatigue or palpitations.
Class IV
Unable to carry on any physical activity without discomfort. Symptoms at rest can be present. If any physical activity is undertaken, discomfort is increased.
- History of long disease process of chronic obstructive pulmonary disease
- Oxygen saturation is less than 88% on room air (02 sat ≤ 88%)
- Patient (p02 ≤ 55 mm Hg)
- Patient (pCO2 > 50 mm Hg)
- Oxygen dependent
- Weight gain or loss related to diagnosis
- Increased emergency department visits or hospitalizations over the past year
- Increased infections or pneumonia during last six months
Secondary Conditions
- Bronchiolitis
- Chronic ischemic heart disease
- Congestive heart failure
- COPD
- Cor pulmonale
- Dehydration
- Emphysema
- Influenza with pneumonia
- Left heart failure
- Pneumonia
- Pulmonary edema
Respiratory Agape Care
Registered nurse: will assess respiratory status, medication efficacy and symptom management related to the pulmonary diagnosis; safety consideration with oxygen usage will be addressed
Social worker: will assist with optimal coping strategies and assist with support related to terminal illness
Spiritual care counselor: will support through listening, presence and prayer based on the patient and family’s needs and beliefs
Home health aide: will perform safe and effective assistive homemaker services
Volunteers: will support with companionship, errands and other activities
- Patient discontinues or is not a candidate for dialysis
- Patient awaiting kidney transplant
- Signs and symptoms associated with renal disease such as: uremia, nausea, preemptive confusion or restlessness
- Creatine clearance less than 10mL/min and serum creatine > 8.0 mg/dl
Secondary Conditions
- Diabetic ascites
- Intractable fluid overload
- May have signs and symptoms of intractable hyperkalemia or oliguria
- Cardiac disease, ascites, congestive heart failure, cachexia
Renal Agape Care
Registered nurse: will manage signs and symptoms of renal failure due to discontinuation of dialysis; comfort and pain management will be obtained
Social worker: will assist patient and family with end -of- life planning to assure wishes are met
Spiritual care counselor: will support based on the patient’s and family’s needs and belief system
Home health aide: will maintain patient’s personal hygiene and assist with activities of daily living
Volunteers: will support with companionship, errands and other activities
- End-stage disease
- Prothrombin time prolonged more than five seconds over control or (INR) > 1.5
- Serum albumin < 2.5 g/Dl
Have at least one of the following
- Ascites despite treatment
- Spontaneous bacterial peritonitis
- Hepatorenal syndrome
- Hepatic encephalopathy despite treatment
- Recurrent variceal bleeding
Supporting Conditions
- Diagnosed hepatitis B or C
- Active ethyl alcohol abuse > 80gm/day
- Muscle wasting
- Undiagnosed viral infections
- Awaiting liver transplant
Registered nurse: will manage signs and symptoms of liver disease; targeted comfort and pain management techniques
Social worker: will provide support for the patient and family with advanced liver disease; assess discomfort and symptom control of ascites pain management and malnutrition
Chaplain: will evaluate end-of-life issues and assist with solutions related to the patient’s belief system
Home health aide and volunteer: will assist with increasing need for assistance with activities of daily living and homemaker chores
Volunteers: will support with companionship, errands and other activities
End Stage Cerebrovascular Accident (ES-CVA)
- Weight loss of more than 10% of body weight during preceding six months
- Weight loss of more than 7.5% of body weight in previous three months
- Serum albumin > 2.5 gm/ dl
- Caloric count documenting inadequate caloric and fluid intake
- Bed-or chair-bound or end-stage CVA
- Karnofsky is less than 40%
Coma
- Persistent vegetative state beyond three days
- Absence of withdrawal from pain
- Physician confirmation related to patient’s non-recovery
- Absent verbal response
- Level of consciousness declined confused or hard to arouse
Secondary Conditions
- Decubitus ulcers
- Multiple infections
- Sepsis
Neurological Agape Care
Registered nurse: will provide comfort and care for the patient with abnormalities who is terminally ill
Social worker: assesses psychosocial issues facing patients with terminal neurological disease; identify illness-related psychiatric conditions
- CD4+ count is less than 25 cell/mcL or viral load is greater than 100,000 copies/mL
And one of the of the following
- Central nervous system lymphoma
- Progressive multifocal leukopenia cephalopathy advanced dementia
- Cryptosporidiosis
- Muscle wasting
- Visceral Kaposi’s sarcoma
- Mycobacterium Avium Complex (MAC), no treatment
- Renal failure, no dialysis
Secondary Conditions
- Serum albumin is> 2.5 g/dL
- Anorexia
- Failure to thrive
- Nausea
- Diarrhea
HIV Agape Care
Registered nurse: will assess for pain and symptom control including new onset infections, nausea and vomiting
Social worker: will provide psychological assessment of patient and family to include adjustment to illness and its complications
Spiritual care counselor: will provide counseling, intervention and support related to that dimension of life
Home health aide and volunteer: will assist with hygiene and comfort maintenance
Volunteers: will provide support and respite as defined by the patient and family
- Severity of dementia > 7A
- Incontinence of either bowel or bladder
- Inability to speak more than six words that are intelligible
- Pyelonephritis
- Septicemia
- Multiple stage-three or-four decubitis ulcers
- Unintentional progressive weight loss of more than 10% of body weight in the last six months
- Multiple emergency department visits or hospitalizations
Secondary Conditions
- Multiple urinary tract infections
- Multiple emergency department visits
Dementia Agape Care
Registered nurse: will assess the patient’s pain or other symptoms related to dementia
Social worker: will assist with caregiver role strain and will facilitate communication with the patient, family and hospice team
Spiritual care counselor: will assist in psychological and spiritual support for the patient and family
Home health aide and volunteer: will assist with personal care and homemaking chores
Volunteers: will assist the family and caregivers to offer relief and respite
FAST score of 7C or greater may be necessary to qualify someone for hospice with diagnosis of dementia. FAST focuses more on the individual’s level of functioning and activities of daily living versus cognitive decline. A person may be at a different stage cognitively (GDS stage) and functionally (FAST stage)
